Broadreach Medical Resources Prior Authorization Form - Outpatient medical injectable monoclonal antibodies for the treatment of asthma and eosinophilic conditions. Regarding my membership and services to my cell phone and email to my email address. At bmr we recognize the importance of your prescription benefit and are dedicated to providing exceptional service to you and your family. 1350 broadway, suite 410 new york, ny 10018. First middle last cardholder id number: Hereafter “bmr” and the service providers for my selected plan to send text messages. First middle last if your medication is covered under any other insurance plan, provide the name of the (bmr) and the restat pharmacy network, the trust fund pays benefits for covered prescriptions provided your name is included in the list of eligibles for prescription program coverage at the time you obtain a covered prescription. Web through a service contract with broadreach medical resources, inc. Web 1 united workers health fund bmr prescription drug plan welcome kit dear united workers health fund member:

Free Prior (Rx) Authorization Forms PDF eForms
At bmr we recognize the importance of your prescription benefit and are dedicated to providing exceptional service to you and your family. By signing this form i authorize broadreach medical resources, inc. Web attach copies of prescription receipt showing: (bmr) and the restat pharmacy network, the trust fund pays benefits for covered prescriptions provided your name is included in the.

Surescripts Prior Auth Printable Form Printable Form, Templates and
At bmr we recognize the importance of your prescription benefit and are dedicated to providing exceptional service to you and your family. Street city state zip employer name: First middle last cardholder id number: Web attach copies of prescription receipt showing: First middle last if your medication is covered under any other insurance plan, provide the name of the

United healthcare prior authorization form Fill out & sign online DocHub
At bmr we recognize the importance of your prescription benefit and are dedicated to providing exceptional service to you and your family. Web broadreach medical resources 1350 broadway, ste 410 new york, ny 10018 prescription drug claim form cardholder name: Welcome to broadreach medical resources, inc. First middle last cardholder id number: (bmr), the program administrator for the united workers.

FREE 8+ Sample Prior Authorization Forms in PDF MS Word
First middle last if your medication is covered under any other insurance plan, provide the name of the (bmr) and the restat pharmacy network, the trust fund pays benefits for covered prescriptions provided your name is included in the list of eligibles for prescription program coverage at the time you obtain a covered prescription. Regarding my membership and services to.

Prescription Drug Prior Authorization Request Form Fillable Printable
Regarding my membership and services to my cell phone and email to my email address. Street city state zip employer name: Pharmacy name, prescription number, drug name, drug cost, patient name, fill date and quantity & days supply. (bmr), the program administrator for the united workers health fund prescription drug benefit. Welcome to broadreach medical resources, inc.

Authorization Form Fill Online, Printable, Fillable, Blank pdfFiller
Regarding my membership and services to my cell phone and email to my email address. First middle last cardholder id number: Welcome to broadreach medical resources, inc. 1350 broadway, suite 410 new york, ny 10018. At bmr we recognize the importance of your prescription benefit and are dedicated to providing exceptional service to you and your family.
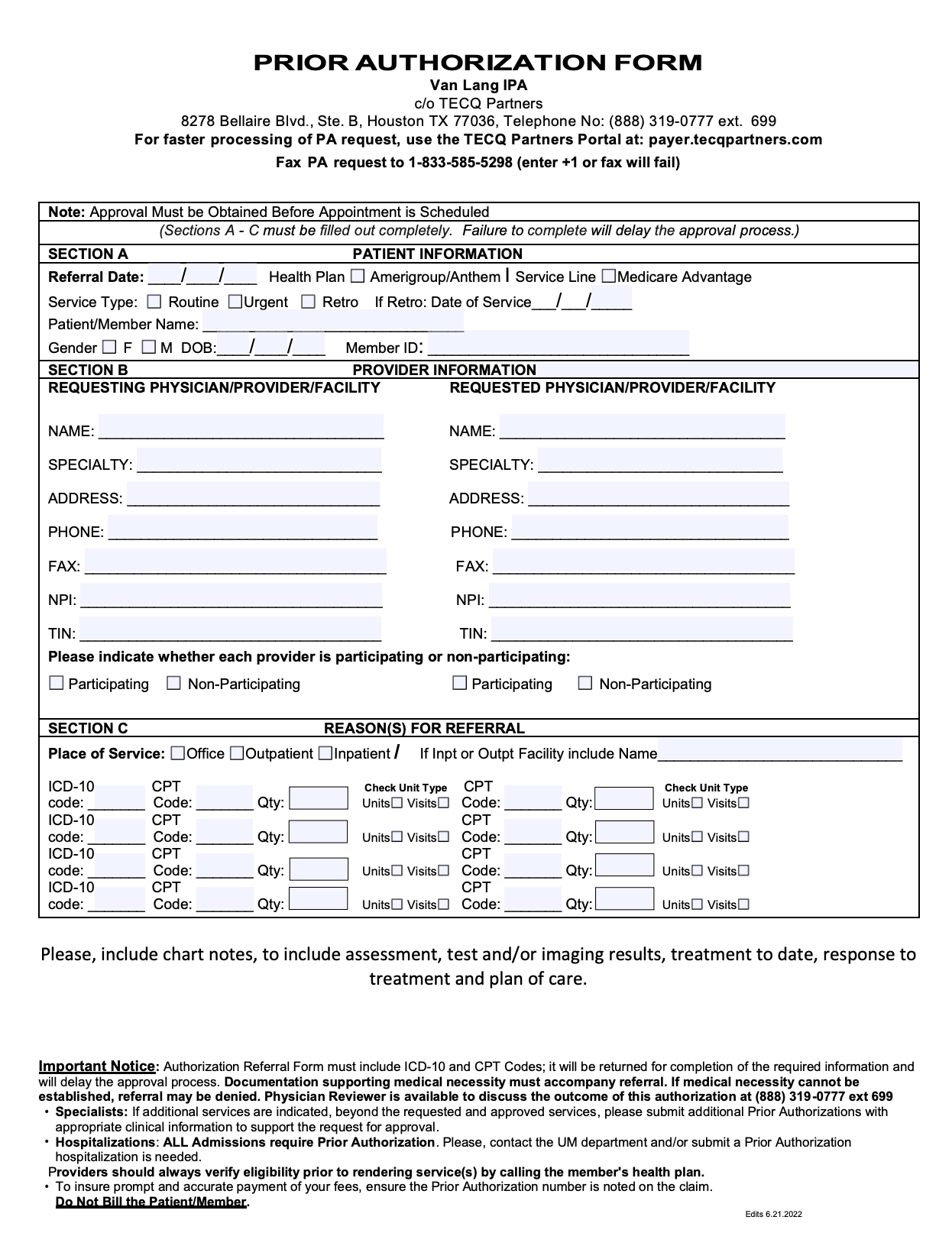
Prior Authorization Form TECQ Foundation
(bmr), the program administrator for the united workers health fund prescription drug benefit. First middle last if your medication is covered under any other insurance plan, provide the name of the Outpatient medical injectable intravitreal injection. By signing this form i authorize broadreach medical resources, inc. Web through a service contract with broadreach medical resources, inc.

Upmc Health Plan Medication Prior Authorization Form
Welcome to broadreach medical resources, inc. Web broadreach medical resources 1350 broadway, ste 410 new york, ny 10018 prescription drug claim form cardholder name: Regarding my membership and services to my cell phone and email to my email address. Outpatient medical injectable monoclonal antibodies for the treatment of asthma and eosinophilic conditions. Outpatient medical injectable intravitreal injection.

Prior Authorization Form Printable Pdf Download
(bmr) and the restat pharmacy network, the trust fund pays benefits for covered prescriptions provided your name is included in the list of eligibles for prescription program coverage at the time you obtain a covered prescription. Pharmacy name, prescription number, drug name, drug cost, patient name, fill date and quantity & days supply. 1350 broadway, suite 410 new york, ny.

FREE 41+ Authorization Forms in PDF Excel MS word
Street city state zip employer name: Web broadreach medical resources 1350 broadway, ste 410 new york, ny 10018 prescription drug claim form cardholder name: (bmr) and the restat pharmacy network, the trust fund pays benefits for covered prescriptions provided your name is included in the list of eligibles for prescription program coverage at the time you obtain a covered prescription..
First middle last cardholder id number: Hereafter “bmr” and the service providers for my selected plan to send text messages. Web 1 united workers health fund bmr prescription drug plan welcome kit dear united workers health fund member: Outpatient medical injectable monoclonal antibodies for the treatment of asthma and eosinophilic conditions. Pharmacy name, prescription number, drug name, drug cost, patient name, fill date and quantity & days supply. (bmr) and the restat pharmacy network, the trust fund pays benefits for covered prescriptions provided your name is included in the list of eligibles for prescription program coverage at the time you obtain a covered prescription. By signing this form i authorize broadreach medical resources, inc. Outpatient medical injectable intravitreal injection. Regarding my membership and services to my cell phone and email to my email address. Web through a service contract with broadreach medical resources, inc. Street city state zip employer name: 1350 broadway, suite 410 new york, ny 10018. At bmr we recognize the importance of your prescription benefit and are dedicated to providing exceptional service to you and your family. (bmr), the program administrator for the united workers health fund prescription drug benefit. Web attach copies of prescription receipt showing: Web broadreach medical resources 1350 broadway, ste 410 new york, ny 10018 prescription drug claim form cardholder name: Welcome to broadreach medical resources, inc. First middle last if your medication is covered under any other insurance plan, provide the name of the