Metlife Change Beneficiary Form - Things to know before you begin: Web beneficiary designation / change. Web change of beneficiary (short form) used to change or designate an individual (s) as your primary or contingent beneficiary (ies). Good order guide and definitions for detailed instructions on completing this form. Life insurance change of beneficiary. For tips on how to complete this form click here. (legal appointment of guardian is required if minor is named as beneficiary.) Request a nursing care provision withdrawal. Metlife metropolitan life insurance company, new york, ny 10166 enrollment change form group customer information (to be completed by the sub code name of group customer/employer wa state health care authority sebb date of hire (mm/dd/yyyy) group customer # report # 219743 branch c] male female coverage effective date. Web this beneficiary change form is provided for your convenience in handling changes or corrections to the beneficiary information for your contract.

Metlife Total Control Account Beneficiary Form 20202021 Fill and
Web use this form to correct, change or designate your beneficiaries. Metlife metropolitan life insurance company, new york, ny 10166 enrollment change form group customer information (to be completed by the sub code name of group customer/employer wa state health care authority sebb date of hire (mm/dd/yyyy) group customer # report # 219743 branch c] male female coverage effective date..

2013 Metlife FEGLI Form FE6 Fill Online, Printable, Fillable, Blank
Make corrections to group participant information. Web this beneficiary change form is provided for your convenience in handling changes or corrections to the beneficiary information for your contract. Things to know before you begin: Metlife metropolitan life insurance company, new york, ny 10166 enrollment change form group customer information (to be completed by the sub code name of group customer/employer.

Life Insurance Beneficiary Form Pdf Fill Online, Printable, Fillable
Your benefits will be paid first to the primary beneficiary(ies). Good order guide and definitions for detailed instructions on completing this form. For tips on how to complete this form click here. Notification of individual name change. Web life insurance change of beneficiary.

Metlife Insurance Change Of Beneficiary Form
Web this beneficiary change form is provided for your convenience in handling changes or corrections to the beneficiary information for your contract. Your benefits will be paid first to the primary beneficiary(ies). Web beneficiary designation / change. Things to know before you begin: If that person(s) is deceased, benefits will be paid to the contingent beneficiary(ies).

20202024 Form MetLife ANNWITHDRAWAL Fill Online, Printable, Fillable
Web life insurance change of beneficiary. If that person(s) is deceased, benefits will be paid to the contingent beneficiary(ies). (legal appointment of guardian is required if minor is named as beneficiary.) For tips on how to complete this form click here. Web change of beneficiary (short form) used to change or designate an individual (s) as your primary or contingent.
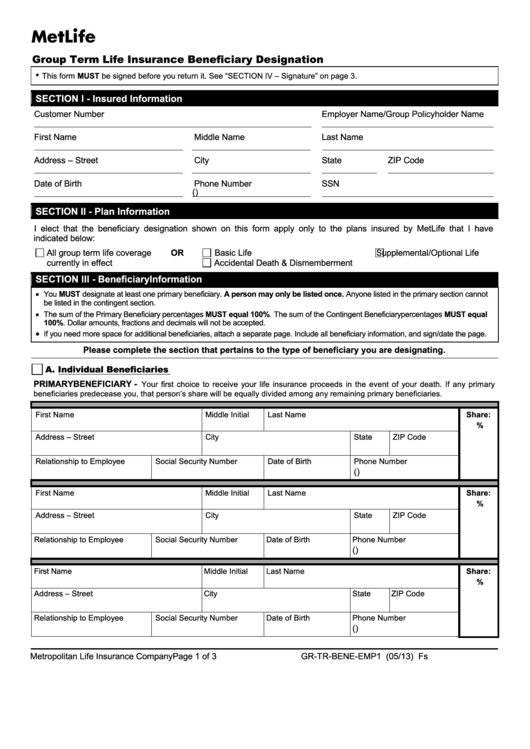
Fillable Form GrTrBeneEmp1 Metlife Group Term Life Insurance
Good order guide and definitions for detailed instructions on completing this form. For tips on how to complete this form click here. For tips on how to complete this form click here. Web beneficiary designation / change. Life insurance change of beneficiary.

MetLife Policy Owner Change Request Form Fill and Sign Printable
Request a nursing care provision withdrawal. Things to know before you begin: Metlife metropolitan life insurance company, new york, ny 10166 enrollment change form group customer information (to be completed by the sub code name of group customer/employer wa state health care authority sebb date of hire (mm/dd/yyyy) group customer # report # 219743 branch c] male female coverage effective.
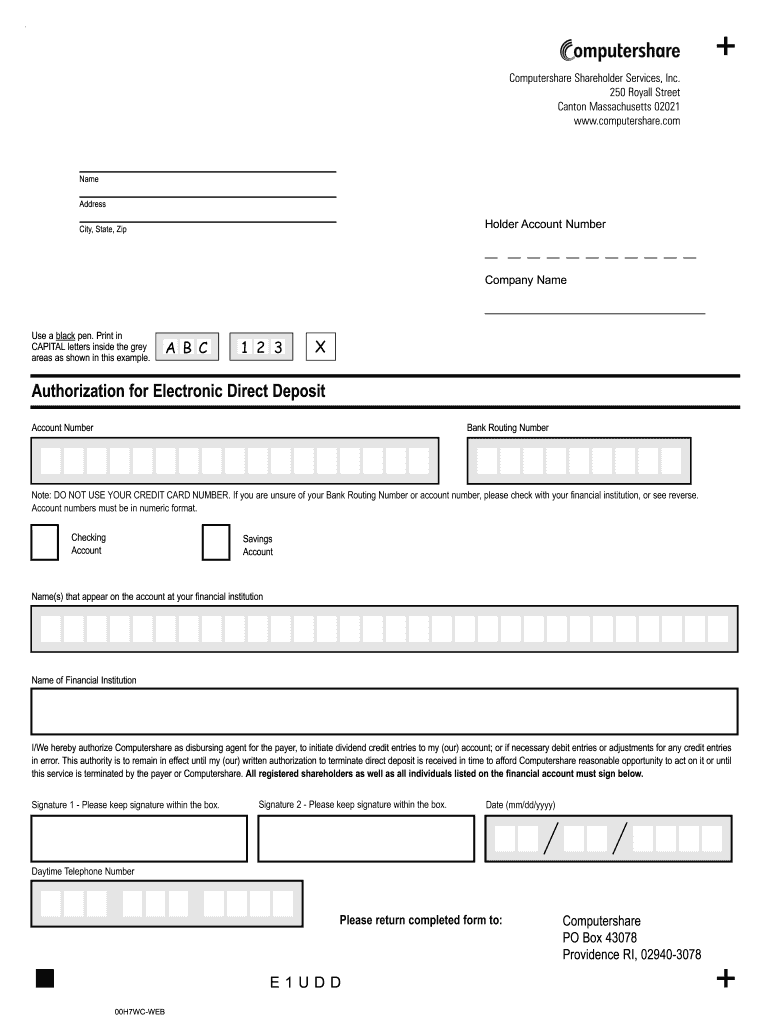
Computershare Metlife Printable Forms Printable Form, Templates and
Life insurance change of beneficiary. Things to know before you begin: Web change of beneficiary (short form) used to change or designate an individual (s) as your primary or contingent beneficiary (ies). Web life insurance change of beneficiary. Web beneficiary designation / change.

Metlife Withdrawal Form ≡ Fill Out Printable PDF Forms Online
Notification of individual name change. Web beneficiary designation / change. (legal appointment of guardian is required if minor is named as beneficiary.) Metlife metropolitan life insurance company, new york, ny 10166 enrollment change form group customer information (to be completed by the sub code name of group customer/employer wa state health care authority sebb date of hire (mm/dd/yyyy) group customer.

Metlife beneficiary change form Fill out & sign online DocHub
Metlife metropolitan life insurance company, new york, ny 10166 enrollment change form group customer information (to be completed by the sub code name of group customer/employer wa state health care authority sebb date of hire (mm/dd/yyyy) group customer # report # 219743 branch c] male female coverage effective date. (legal appointment of guardian is required if minor is named as.
(legal appointment of guardian is required if minor is named as beneficiary.) For tips on how to complete this form click here. Web use this form to correct, change or designate your beneficiaries. Good order guide and definitions for detailed instructions on completing this form. Web life insurance change of beneficiary. Life insurance change of beneficiary. Notification of individual name change. If that person(s) is deceased, benefits will be paid to the contingent beneficiary(ies). Web this beneficiary change form is provided for your convenience in handling changes or corrections to the beneficiary information for your contract. Web change of beneficiary (short form) used to change or designate an individual (s) as your primary or contingent beneficiary (ies). Make corrections to group participant information. Your benefits will be paid first to the primary beneficiary(ies). Metlife metropolitan life insurance company, new york, ny 10166 enrollment change form group customer information (to be completed by the sub code name of group customer/employer wa state health care authority sebb date of hire (mm/dd/yyyy) group customer # report # 219743 branch c] male female coverage effective date. Web beneficiary designation / change. Request a nursing care provision withdrawal. For tips on how to complete this form click here. Things to know before you begin: