Release Of Information Form Template Mental Health - Web authorization for the release of information is not sufficient for this purpose for client records applicable under federal law 42 cfr part 2. Web release of information consent form 1. Web authorize [insert name of mental health counseling organization] to disclose to and/or obtain from: Patient information patient full name: I authorize ellie mental health 1370 mendota hts rd mendota hts, mn 55120 phone: Previous treating therapist, current health care providers, parents or school) client name(s): Web the protected health information indicated below with: _____ patient date of birth: I, the undersigned, understand that a copy of this signed authorization form is as acceptable as the original. ☐assessment ☐care plan ☐individual therapy notes ☐med notes

Free Mental Health Release Of Information Form
I authorize the release of any and all of the following medical, mental health and/or substance use disorder information, as specified, which may be contained in my records (check all that apply)with the following date parameters: Web this authorization is for: Patient information patient full name: Web authorization for release/exchange of information. Previous treating therapist, current health care providers, parents.

30 Medical Release Form Templates ᐅ Templatelab Mental Health Release
Form of disclosure unless you have specifically requested in writing that the disclosure be made in a certain format, we reserve the Patient information patient full name: Web release of information consent form 1. Web this authorization is for: I authorize the release of any and all of the following medical, mental health and/or substance use disorder information, as specified,.

Free Release Of Information Template
_____ patient date of birth: Web authorize [insert name of mental health counseling organization] to disclose to and/or obtain from: Web authorization for the release of information is not sufficient for this purpose for client records applicable under federal law 42 cfr part 2. ☐assessment ☐care plan ☐individual therapy notes ☐med notes Web mental health treatment i, _____[insert name of.

FREE 9+ Sample Release of Information Forms in MS Word PDF
I, the undersigned, understand that a copy of this signed authorization form is as acceptable as the original. Form of disclosure unless you have specifically requested in writing that the disclosure be made in a certain format, we reserve the The protected health information to be disclosed includes the following: Web this authorization is for: Patient information patient full name:

Medical Release of Information Form Fill Out, Sign Online and
Patient information patient full name: Web mental health treatment i, _____[insert name of patient/client], whose date of birth is _____, authorize [insert name of social work organization] to disclose to and/or obtain from: I, the undersigned, understand that a copy of this signed authorization form is as acceptable as the original. I authorize the release of any and all of.
Sample Release Of Information Form Mental Health Classles Democracy
The protected health information to be disclosed includes the following: ☐coordination of care ☐legal ☐personal ☐other (must specify) _____ information to be disclosed: Form of disclosure unless you have specifically requested in writing that the disclosure be made in a certain format, we reserve the This form provides your therapist with written permission to communicate with other individual providers regarding.

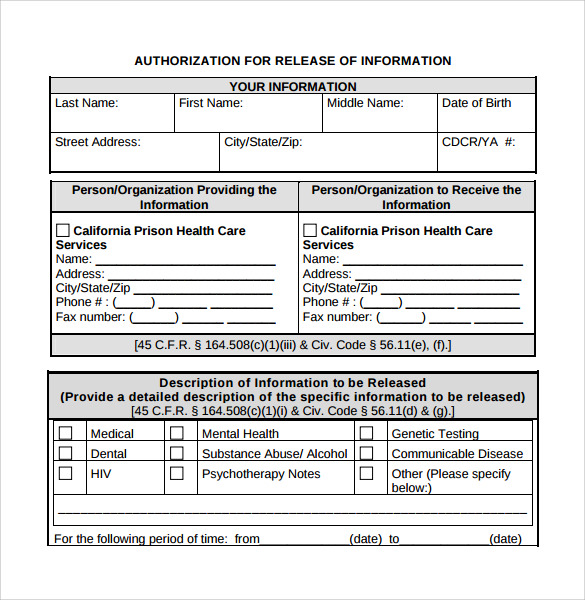
Mental Health Release Of Information Form California
Web authorization for the release of information is not sufficient for this purpose for client records applicable under federal law 42 cfr part 2. I authorize the release of any and all of the following medical, mental health and/or substance use disorder information, as specified, which may be contained in my records (check all that apply)with the following date parameters:.

FREE 17+ General Release of Information Forms in PDF Ms Word
Form of disclosure unless you have specifically requested in writing that the disclosure be made in a certain format, we reserve the Web mental health treatment i, _____[insert name of patient/client], whose date of birth is _____, authorize [insert name of social work organization] to disclose to and/or obtain from: ☐assessment ☐care plan ☐individual therapy notes ☐med notes ☐coordination of.

FREE 47+ Printable Release Form Samples & Templates in PDF MS Word
Web authorization for the release of information is not sufficient for this purpose for client records applicable under federal law 42 cfr part 2. Patient information patient full name: Web this authorization is for: Web the protected health information indicated below with: I, the undersigned, understand that a copy of this signed authorization form is as acceptable as the original.

Mental Health Release Of Information Form Template
I authorize the release of any and all of the following medical, mental health and/or substance use disorder information, as specified, which may be contained in my records (check all that apply)with the following date parameters: _____ patient date of birth: [insert name of person or title of person or organization] description of information to be disclosed Previous treating therapist,.
Web authorization for the release of information is not sufficient for this purpose for client records applicable under federal law 42 cfr part 2. This form provides your therapist with written permission to communicate with other individual providers regarding your treatment (e.g. Web release of information consent form 1. [insert name of person or title of person or organization] description of information to be disclosed I, the undersigned, understand that a copy of this signed authorization form is as acceptable as the original. Previous treating therapist, current health care providers, parents or school) client name(s): Form of disclosure unless you have specifically requested in writing that the disclosure be made in a certain format, we reserve the ☐assessment ☐care plan ☐individual therapy notes ☐med notes ☐coordination of care ☐legal ☐personal ☐other (must specify) _____ information to be disclosed: I authorize the release of any and all of the following medical, mental health and/or substance use disorder information, as specified, which may be contained in my records (check all that apply)with the following date parameters: Web authorize [insert name of mental health counseling organization] to disclose to and/or obtain from: I authorize ellie mental health 1370 mendota hts rd mendota hts, mn 55120 phone: Patient information patient full name: Web mental health treatment i, _____[insert name of patient/client], whose date of birth is _____, authorize [insert name of social work organization] to disclose to and/or obtain from: Web this authorization is for: _____ patient date of birth: Web authorization for release/exchange of information. The protected health information to be disclosed includes the following: Web the protected health information indicated below with: